

Five Strategies for Securing Acquittal in Physician Opioid Prescribing Cases - Post Ruan
The Supreme Court’s Decision in Ruan v. United States
In the landmark 9-0 decision in the case of Ruan v. United States the Supreme Court rejected the Department of Justice’s efforts to hold a physician to a “objective” standard of care regardless of the physician’s intent in prescribing. Instead, Justice Breyer determined that the elements if 21 U.S.C. 841(a) and 21 C.F.R. 1306.04 require the government to prove that the physician “knowingly and intentionally” prescribed for other than a legitimate medical purpose. While the Government hoped for jury instructions in “pill mill” cases that instruct the jury it can convict a physician for a mere violation of the standard of care - whether or not the conduct was intentional drug trafficking - their efforts failed.
To understand more about the Ruan decision, read this. The importance of Ruan is that the subjective intent of the physician still matters in opioid prosecutions. The well-intended physician who seeks in good faith to treat patients can introduce evidence of their “good faith” regardless if their prescriptions fell outside the government’s version of objective prescribing requirements such as the CDC Guidelines, ASIPP Guidelines, and FSMB Guidelines.
While the victory was an incredible achievement for patient advocates, the defense bar, and providers facing scrutiny, many are left wondering if the impact of the decision will be felt in further Government prosecutions for overprescribing controlled substances. Immediately after the decision, defense attorneys around the country were effectively scratching their head to determine the impact of the decision and how their case may change. Here are five essential strategies that will aid in securing a defense acquittal in opioid prescribing cases against physicians post Ruan.
Five Essential Post Ruan Trial Strategies
I have been fortunate to earn an acquittals in several prominent opioid prescribing prosecutions including:
Another case, United States v. Naum, was recently vacated by the Supreme Court as a result of the Ruan decision because the judge incorrectly conflated the criminal standard with the “standard of care”. Building on successful verdicts, this article is intended to assist the practitioner and physician facing scrutiny with the evidence and trial skills necessary to achieve acquittal in a post-Ruan environment. These victories were the result of a team of people all working together to create a picture of appropriate prescribing and a full fledged attack on the government’s use of rigid and objective standards to apply to the practice of medicine. Below are my five trial strategies that will increase the chances of a successful outcome.
An Exhaustive Internal Investigation at the Outset of the Case
Had I not met the team of talented experts at CCG Healthcare, the list above would be much much shorter. CCG maintains a team of compliance experts, controlled substance prescribing experts, former federal law enforcement (including DEA), former medicare/medicaid investigators etc. In an environment where defense investigators generally know very little about healthcare - CCG investigators hit the ground running and know exactly where the Government is going to look for evidence of problematic prescribing.
At the earliest stage of a case, I involved CCG to review records in question, review undercover video, interview employees and local providers to generate a volume of information that has, in many cases, surpassed the government’s knowledge. They know the typical “red flags” made at issue by the government and his ability to internally investigate the source of the problem and aid the physician in taking corrective action provides both an exculpatory and mitigating angle to the case that has made his efforts indispensable.
An exhaustive internal investigation is a must for any physician facing scrutiny. The old adage about letting sleeping dogs lie and not pissing off the government by doing an investigation is an old and tired way of thinking in the current regulatory space. DOJ and OIG policy doesn’t just request that the provider do an internal investigation at the first sign of wrongdoing - it demands it. Whether you utilize the skills and abilities of CCG or have your own healthcare investigator - you need to review records, get everyone interviewed, and develop exculpatory and mitigating evidence as early in the case as possible.
CCG’s investigation generally follows the following format:
Identify records reviewed by the government,
Review records to determine areas of concern,
Interview all employees,
Interview positive patient witnesses,
Interview patients at issue,
Audit the practice and suggest corrections to compliance shortfalls.
2. Statistical Analysis
Its no secret that the Government uses data mining to find targets for opioid and healthcare fraud prosecutions. Often criminal referrals are of the top prescribers in a state and search warrants are conduct to confirm what the prosecutors believe they already know based on prescribing and billing data. But we all know that data can be spun in many different ways and utilized for many different purposes. In this modern age, data analytics is essential to understanding your client’s prescribing and billing habits, potential culpability, and as an investigative tool guiding further investigation. Moreover, analytics can provide powerful acquittal evidence. Take this case study for example.
In United States v. Bothra et. al. the prosecution claimed that physicians hooked patients on powerful narcotics in order to get them to submit to expensive and “unnecessary” interventional procedures. They claimed that all patients were treated the same and that the procedures were unnecessary.
Utilizing CCG Healthcare’s statistical analytics capability we were able to completely disprove the Government’s theory with minimal effort. Lets take a look at the graphs that were shown to the jury.
Context is important here. In the Bothra case we knew that the government had to show that injections were tied to opioids. If their theory was correct, you would see a correlation between injections and opioids. You would also see that the treatment varied little on a patient by patient basis. Also, as one could imagine, if that was the scheme, you would see that most patients got opioids and continued treatment at the practice for a long period of time.
After utilizing CCG Healthcare’s data analytics capability - it was abundantly clear that the Government’s position was not supported by the evidence.







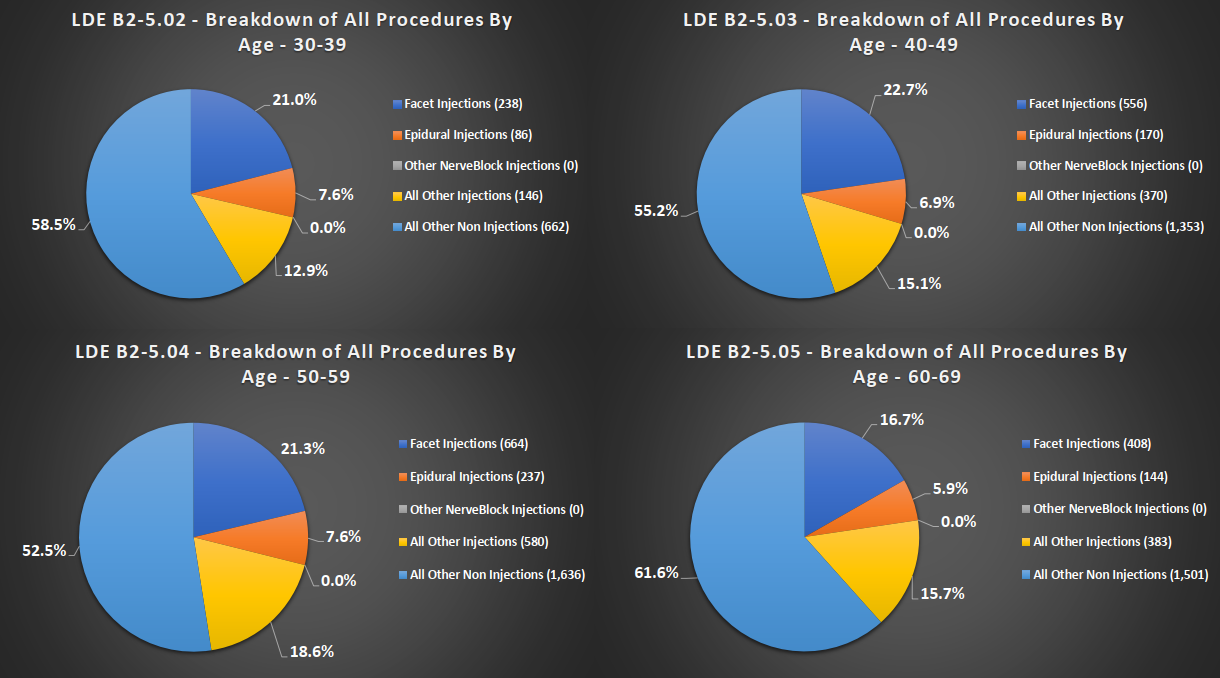

After reviewing the charts, you can see that many patients were not prescribed opioids. Further, the average number of visits for patients was relatively low - just one or two in a 90 day window. In addition, the selection of opioid varied greatly and treatment was anything but “cookie cutter”.
The Government couldn’t argue with this evidence. It did not introduce statistical evidence of its own and as a result of the strength of the data analysis - we argued that the government proceeded through their investigation with “blinders” on and decided to remain willfully blind of the actual evidence in the case. The jury came back with a full acquittal on all 54 counts.
3. Cross Examination of the Government’s Expert
The most pivotal moment in any unlawful prescribing or opioid prosecution is the cross examination of the Government’s expert.
This issue is more fully discussed here.
The most successful attacks against the opposing expert testimony is the standard applied and the selection of patient
files. Most government experts choose to point out red flags and deviations of the standard of care including failure to recognize inconsistent urine drug screens,
poor documentation, failure to conduct a physical examination, and improper history and physical. While problematic, the issues outlined above are not determinative of bad faith in prescribing. The expert’s methodology should be challenged during motions practice. The trial court must determine whether an expert’s testimony rests on a reliable foundation and is relevant to the “task at hand.” An expert witness who only relies on his or her own subjective view of proper medicine and does not adhere to a
standard should not meet this test. Moreover, Gonzales v. Oregon makes clear that the structure and operation of the CSA presume and rely upon a functioning medical profession regulated under the states’ police powers. Therefore, the government expert should adhere to a state standard for determining the bounds of professional practice. If the government expert fails to apply a common standard applicable to the defendant prescriber, the expert should be challenged on the fact that his or her subjective belief and independent review of literature are hardly the basis for a statewide minimum standard of practice. Cross examination begins with a Daubert challenge of the expert’s review and utilization of documents that are not “standards of care” but rather guidelines such as the CDC Guidelines, ASIPP Guidelines, FSMB Guidelines and state prescribing guidelines. If an expert bases the totality of their review on these guidelines amalgamated into some sort of standard - a Daubert challenge is ripe.
Next, the practitioner must be ready to spar with the expert on the medicine that is practiced. Obtain pain management textbooks, understand drug metabolites, urine drug screen results, dangerous drug combinations, CDC guidelines, and FDA warnings. Research every opinion contained in the expert report and find authoritative resources that rebut the allegations.
Click here for a sample Daubert challenge in the Defense Acquittal in United States v. Bothra et. al.
Additionally, cross examination can be aided by a defense investigation into the expert, their practice, and their medical records. In the case of United States v. McCutchen, we obtained medical records authored by the expert who was very critical of the Defendant’s medical records. We were able to show that the “expert” made many of the mistakes that the defendant made and that his analysis was hypocritical. A talented healthcare investigator such can provide you an edge during cross examination by pulling prescribing data, prior records, prior transcripts and even a bit of undercover work to determine the expert’s true nature.
Rather than attempting to draft a play by play cross examination that is likely to be fruitless, I have attached cross examinations of experts in my recent acquittals. Each was a unique and fact intensive exploration of the expert’s qualifications, opinions, and oversights. The one common theme between each was an inquiry into the standard utilized by the expert. Most prosecutors muddy the clear demarcation between “standard of care” and “outside the usual course of professional practice for other than a legitimate medical purpose”. This is obviously because its easier to convict a physician by applying a rigid “standard of care” developed from the mind of the government’s expert. However, this is improper - especially in light of Ruan v. United States which eschews the application of a rigid standard of care in favor of evidence of intent to violate the requirements of a DEA registration.
Sample Cross Examinations
Cross Examination of Dr. Stephen Thomas in the Defense Acquittal United States v. Aggarwal et. al.
Cross Examination of Dr. Neil Mehta in the Defense Acquittal in United States v. Bothra et. al.
Cross Examination of Dr. Carl Christensen in the Defense Acquittal in People v. Oesterling
4. Jury Instructions
Jury instructions are perhaps more important in opioid prosecutions than any other area of criminal law. Opioid prosecutions are the only area of criminal law in which the jury is tasked with understanding concepts such as “standard of care” and legitimacy of treatment without the aid of the civil compulsory and discovery tools our civil counterparts are used to. This is all done under the backdrop of a standard that is not defined by statute and left up to the vague ambiguous words of a regulation that offers no parameters of conduct informing the jury and the physician of the range of permissible conduct.
Jury instructions were the central issue in Ruan, and while the Supreme Court stopped short of providing a proper jury instruction to the Circuit’s, it did reject the application of an objective test to determine the criminality of prescribing.
The instruction in Ruan read as follows:
A controlled substance is prescribed by a physician in the usual course of a professional practice and, therefore, lawfully if the substance is prescribed by him in good faith as part of his medical treatment of a patient in accordance with the standard of medical practice generally recognized and accepted in the United States. The defendants in this case maintain at all times they acted in good faith and in accordance with [the] standard of medical practice generally recognized and accepted in the United States in treating patients. Thus a medical doctor has violated section 841 when the government has proved beyond a reasonable doubt that the doctor’s actions were either not for a legitimate medical purpose or were outside the usual course of professional medical practice.
The issue with this instruction, according to Ruan’s counsel, is that the instruction fell short of advising the jury that the defendant’s good faith in prescribing was sufficient for an acquittal. In other words, the instruction did not go far enough to establish that the physician must have knowingly prescribed for other than a legitimate medical purpose.
Instead, Ruan proposed the following instruction which advised the jury that “good faith” was sufficient for acquittal:
Good faith in this context means good intentions and the honest exercise of professional judgment as to the patient’s needs. It means that the Defendant acted in accordance with what he reasonably believed to be proper medical practice.
Again, the Supreme Court did not specifically uphold a “good faith” instruction. However, practitioners must continue to fight for a “good faith” instruction in order to permit a jury to differentiate between the criminal physician and the well intended but poorly educated or careless physician. Carelessness is a matter for the medical board and not deserving of decades in jail.
I had the pleasure of being involved in the first post Ruan case in which a judge was required to navigate instructions after interpreting Ruan absent the 6th Circuit’s say on the issue. The instructions are included here. The problem with this instruction is that it does not include a “good faith” instruction. The trial judge felt that it was inappropriate and believed that simply parroting the statutory elements and justice Breyer’s burden shift was sufficient.
The gold standard instruction in the 9th Circuit developed in the case of United States v. Feingold remains the most defense friendly jury instruction which will likely be revitalized among the circuits. The Feingold instruction should be pursued by defense counsel post Ruan because it ensures that the jury will not mistake the criminal standard for the malpractice standard and convict a physician for a violation of the “standard of care”.
While the judge is responsible for instructing the jury on the law, counsel should remind the jury that malpractice is insufficient to convict repeatedly through the trial. Below is a helpful slide I use to inform the jury of the difference between the “best practices” and conduct that is “outside the bounds of professional practice”.
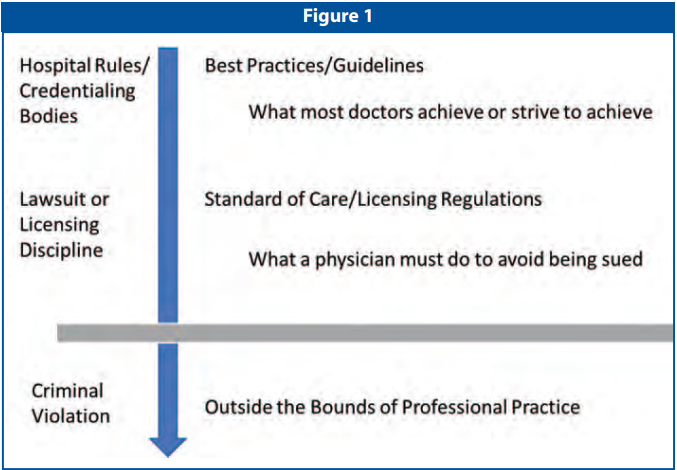
Slide showing the difference between “best practices” and the criminal standard
5. Client Testimony
Defendant testimony is vital to securing an acquittal.
The jury wants to hear from the doctor and failure to call the Defendant to testify will certainly lead to an adverse inference against the Defendant. While it is true that the judge instructs the jury that the Defendant need not take the stand, the jury will be left without the physician’s perspective. In a post Ruan environment, this means that the jury will not get a sense of the Defendant’s reasons for prescribing. Most physicians facing prosecution for violating 21 U.S.C. 841(a) find themselves the target of a federal prosecution because they were trying to do their best under difficult circumstances. They may have not had sufficient controlled substance training, been too naïve, they may be elderly or possibly exhibit more compassion than other doctors leading them to accept patients that others will not. The jury needs to be able to see the physician and understand their character in order to see the difference between the evil drug dealer the government will make them out to be.
When testifying, the defendant should lay a solid foundation of their background, training, family life, and reasons for practicing medicine. If the physician faced challenges in private practice - bring them to light. The jury understands that people are fallible and may struggle running a business or practice. Next, the physician must know the medicine better than anyone in the courtroom and have sufficient justification for each prescription written. We are not confined to the medical record during this exercise. The physician can supplement the records with information that he or she is aware of that aided in the prescribing decision.
Finally, the Defendant should be treated as a quasi expert and provide information to the jury that rebut the government’s claims. For instance, in a recent case where the government introduced evidence that the physician ignored the results of urine drug tests, the physician provided a study to the jury indicting that the urine drug screen should not be utilized as a punitive tool and is not solely a basis to make a medical determination. Often, the government argues that a “negative” urine drug screen is an indication of unlawful diversion. This physician knew this wasn’t true and testified that often patients taking pain medication “as needed” have a negative urine drug test result. Moreover, he discussed studies which showed that small amounts of hydrocodone and oxycodone can leave the system in as little as 8 hours.
Client testimony is vital in ensuring that the jury is able to peer into the mind of the physician and understand the reasonableness of prescribing practices. A client’s willingness to testify factors heavily in my decision whether or not to advise my client to proceed to trial.
Conclusion
A strong defense in any 21 U.S.C. § 841 prosecution against a prescriber requires a narrowing of the standard, solid expert testimony, and a strong presentation of the patient’s medical need for the prescriptions issued by the physician. Federal prosecutions are shifting toward prosecution for mere violations of the standard of care. It is imperative that the defense bar reject any effort to charge and subsequently convict a physician for deviations from the standard of care. It must remain the case that to convict a physician for a violation if 21 U.S.C. § 841(a), the physician must have ceased practicing medicine and instead engaged in illicit drug trafficking.